Human health services are the reverse of software and audiovisual services. The service itself is not the IP right. Instead, IP sits upstream in medicines, devices, software and data, shaping what the health system can buy, use and deliver. New Zealand has kept health services outside its GATS commitments, but that does not mean the sector is outside trade policy. It means the pressure arrives through the IP layer instead of the services schedule.
1. Health Services in New Zealand’s Economy
Health providers are heavy users of confidentiality and modest users of formal IP rights. That is consistent with the structure of the sector. The clinics, hospitals, practices and care providers that appear in the Business Operations Survey do not hold pharmaceutical patents; they consume patented inputs from manufacturing sectors. The result is a conspicuous asymmetry between the IP that enables the service and the IP that appears inside the service sector itself.
The pattern is striking. Health care and social assistance firms rely overwhelmingly on confidentiality agreements, while patents are close to absent. That does not mean health is low-tech. It means the relevant patents sit outside the service sector, in pharmaceuticals, devices and software supply chains. The chart therefore captures the service end of the health economy, not the upstream patent-heavy manufacturing end.
The time series shows a stable pattern of confidentiality-led protection and a low patent share. That is consistent with the sector’s role as a user of medicine, data and software rather than a producer of patentable health inputs.
2. What the IP–Services Toolkit Shows
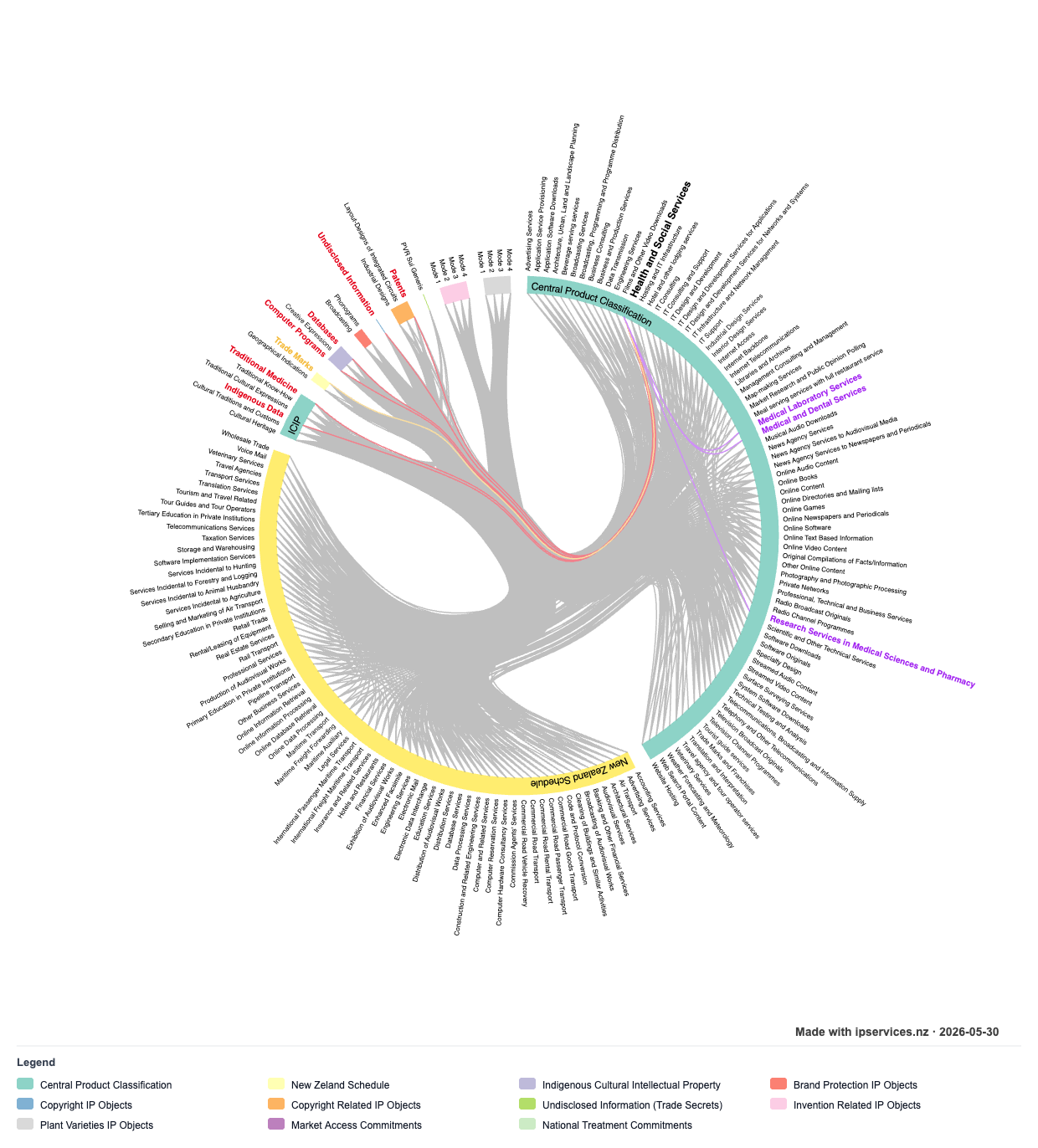
The IP–Services Toolkit would map health services to a different kind of dependency chain from the direct-linkage studies. The service sits outside New Zealand’s GATS schedule, but the surrounding input structure still matters. Patents and invention-related rights govern pharmaceuticals and medical devices upstream; data exclusivity and data protection govern clinical data; computer programs govern management systems, diagnostics and telehealth; traditional medicine and traditional knowledge sit close to Māori health practice; and trade marks distinguish branded medicines from generic medicines.
3. Interface Layers
Three interface points explain why health services remain exposed to trade-related IP settings even without a services commitment. First, pharmaceutical patents and regulatory data rules shape the timing and affordability of medicine access. Secondly, software licensing and cross-border data governance shape how digital health tools can be deployed in practice. Thirdly, traditional knowledge protection determines whether culturally grounded health practice can be used on fair terms. Taken together, these layers show that practical health-system access is governed by legal design upstream of the service itself.
3.1 Pharmaceutical patents and data exclusivity
The main IP pressure in health is not inside the service sector. It arrives through the medicines and devices that the sector depends on. Negotiating models only work if generic medicines can enter when patent protection expires, or earlier where TRIPS flexibilities are used.
That is why pharmaceutical patents and data exclusivity matter so much. Patent expiry opens the door to generic medicines. Data exclusivity can keep that door partly shut even when patent protection has fallen away, because the regulatory data file for a new medicine may remain unavailable to competitors. For biologics, that issue is especially sharp. Comparative work on patent law and regulatory data exclusivity describes this as institutional "mission creep": where tighter patentability standards can shift strategic protection pressure into data exclusivity regimes, with direct implications for medicine access and health-system costs.[1] Moreover, data exclusivity design is a decisive variable in pharmaceutical access and competitive entry conditions.[2]
New Zealand’s health policy therefore depends on a trade policy balance that is wider than services market access. The central question is not whether a foreign hospital can establish itself here. It is whether New Zealand can maintain affordable supply of the medicines that make health services usable in practice.
3.2 Health technology, diagnostic software and cross-border data
Modern health services are digital. Electronic health records, telehealth platforms, diagnostic tools and clinical decision software all sit within copyright, database control and software licensing. That makes the health sector a consumer of computer services as well as a consumer of medicines.
The legal issue is about access. A health provider may have lawful access to a tool, yet still be constrained by licence conditions, platform lock-in or data-handling terms that sit outside the health services regime. The rise of AI-assisted diagnostics makes this sharper, because the training data, the model, the user interface and the resulting recommendation may each be governed by different rights or contracts. This operational view of IP governance emphasises how licensing design and information control shape what firms and institutions can do in practice.[3]
Cross-border data flow rules add another layer. Health data sovereignty matters for privacy, safety and trust, but digital trade disciplines in modern FTAs can make data localisation harder to insist upon. That does not remove the regulatory concern, but just shifts it into the trade law architecture.
The outward-facing side is equally important. New Zealand suppliers of digital health tools, clinical software and related services can face destination-market data localisation requirements, regulatory data constraints and approval pathways that condition cross-border supply as strongly as headline services commitments.[4] Export performance in health-linked services therefore turns on regulatory operability across jurisdictions rather than market-access language alone. Therefore, technology transfer and practical access conditions are as important as formal rights design when systems face global stressors such as pandemics.[5]
3.3 Traditional medicine and knowledge protection
Health is also where the traditional knowledge question comes into light. Rongoā Māori is both a health practice and a repository of traditional knowledge. It is valuable because it is embedded in Māori community practice, yet that same quality makes it hard to protect through ordinary IP rules.
The risk is familiar. A firm can take a plant-based formulation or a healing practice, isolate the useful ingredient, and seek legal protection in a way that ignores its traditional source. The ordinary patent system can reward the later extractor more easily than the earlier knowledge holder.
This is where the broader policy problem becomes visible. If health is to be treated as a trade policy issue, then the treatment of medicines, data and traditional medicine cannot be separated. They are different parts of the same supply chain. This is a cross-cutting policy question: traditional knowledge requires interface and defensive strategies that operate across legal and institutional settings rather than inside a single IP right.[6]
4. Takeaway
Human health services are outside New Zealand’s GATS schedule, but not outside the reach of trade-related IP rules. The sector depends on patented medicines, protected clinical data, software licences and the legal treatment of traditional knowledge. The BOS data shows the service-side end of that system: low patent use, high confidentiality and little direct IP ownership.
Accordingly, the policy frame must run both ways: New Zealand’s internal settings shape conditions for inbound suppliers and system resilience, while New Zealand health-linked exporters face parallel IP-data bottlenecks abroad.
The lesson is that a blank services schedule does not equal a blank policy field. The real pressure sits upstream. If New Zealand wants health services to remain affordable, available and culturally grounded, it has to read the IP chapter and the health system together.
Jessica Lai and Susy Frankel "Patent Law and Regulatory Data Exclusivity: Game Playing and 'Mission Creep'" in Christophe Geiger (ed) The Interface of Intellectual Property Law with Other Legal Disciplines (Edward Elgar, 2025) 52. ↩︎
Khushbu Kumari "Reassessing the Data Exclusivity Regime for the Indian Pharmaceutical Industry" (PhD thesis, Te Herenga Waka—Victoria University of Wellington, 2024) https://doi.org/10.26686/wgtn.25857238. ↩︎
Susy Frankel and Rory McLeod Intellectual Property Law and Policy: A Primer (NZPECC, 2025) ch 2.8 and ch 5.4 <www.nzpecc.org.nz>. ↩︎
Nikita Melashchenko "Data Barriers to International Trade" (PhD thesis, Te Herenga Waka—Victoria University of Wellington, 2022) https://doi.org/10.26686/wgtn.20443746. ↩︎
Susy Frankel "International Intellectual Property, Innovation, Technology Transfer and Sustainable Development" in Christophe Geiger (ed) Intellectual Property, Ethical Innovation and Sustainability: Towards a New Social Contract for the Digital Economy (Edward Elgar, 2025) preprint available at https://dx.doi.org/10.2139/ssrn.5513818. ↩︎
Frankel and McLeod, above n 3, ch 2.4 and ch 5.1.3. ↩︎